Smita Bhatia, MD, MPH
- Professor and Chair
- Department of Population Science
- City of Hope
- Duarte, California
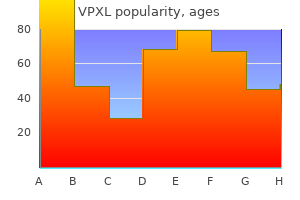
VPXL dosages: 12 pc, 9 pc, 6 pc, 3 pc, 1 pc
VPXL packs: 12 month supply, 9 month supply, 6 month supply, 3 month supply, 1 month supply
Vpxl 1 pc cheap amex
Shortening and malrotation may be readily assessed on the finish of the procedure and corrected instantly by revising placement of the proximal interlocking screw or screws. Selecting larger-diameter nails based on feedback of cortical chatter during reaming seems to improve union rates when the retrograde nailing approach is used. Epidemiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965�1984. Identification of the optimum intercondylar place to begin for retrograde femoral nailing: an anatomic research. Paying close consideration to the right nail insertion starting point and guaranteeing that the distal portion of the nail remains subchondral are two key technical points to avoiding potential knee issues. Use of an interlocked cephalomedullary nail for subtrochanteric fracture stabilization. Ipsilateral fractures of the femur and tibia: treatment with retrograde femoral nailing and unreamed tibial nailing. Retrograde intramedullary nailing, without reaming, of fractures of the femoral shaft in multiply injured patients. Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. Prospective comparability of retrograde and antegrade femoral intramedullary nailing. Neurologic and vascular constructions at risk during anterior-posterior locking of retrograde femoral nails. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: enchancment with a standard protocol. Meniscal damage related to femoral shaft fractures: an arthroscopic analysis of incidence. Some fracture strains prolong proximal or distal to the shaft and are due to this fact not considered shaft fractures. This description is mostly semantic, as the more important facet of definition is understanding the "character" of the fracture. Fractures whose important factor is diaphyseal with "extensions" into the outer regions are completely different than fractures whose essential factor is subtrochanteric or supracondylar with extension into the diaphysis. In some circumstances there could also be enough involvement of proximal or distal features that remedy should change. Open fractures are often graded in accordance with the GustiloAnderson classification, but one must keep in mind that this classification system was designed for the tibia, a subcutaneous bone. Thus, if absorbed vitality is taken into account, theoretically, considerably extra vitality can be required to fracture a femur and disrupt the gentle tissue envelope around a femur than round a tibia. Nonetheless, this system is extensively employed within the femur for descriptive functions. Surgical options for such irregular bowing embrace plate fixation or a managed osteotomy to permit nail placement. Normal aging and osteoporosis leads to a biomechanical adaptation of enlarged internal diameter. Thus, aged people may have a larger-diameter femoral shaft with a thinner cortex. As in different cylindrical tubes, the bending rigidity of the femur is roughly proportional to the radius to the fourth energy. The vascular supply to the femur is from a nutrient artery off the second perforating department of the profunda femoris, entering posteriorly alongside the linea aspera. Normally, periosteal branches provide the outer one quarter to one third of the cortex as the course of blood move is centripetally outward from the medulla to the cortex. Once fracture occurs, a reversal of blood flow occurs from the periosteal vessel, radially inward. The linea aspera protects many perforating periosteal vessels, except in extreme fractures, and may assist clarify the high healing price of femoral shaft fractures (about 95%).
Vpxl 12 pc buy mastercard
The fracture pattern can differ from the simplest extra-articular kind to probably the most complicated intra-articular harm. Owing to the gastrocnemius complex, an apex posterior deformity of the condyles occurs because the fragments are flexed because of the muscle attachment. The patient presents with a swollen and tender knee after both a fall or some high-energy trauma (motor automobile or motorbike accident). Any attempts at range of movement result in extreme ache, and significant crepitus is normally famous with palpation. The physical examination is directed primarily at ascertaining the neurovascular standing of the lower limb and figuring out whether any associated accidents exist, especially the hip (see Exam Table for Pelvis and Lower Extremity Trauma, pages 1 and 2). If there are any small wounds or tenting of the skin anteriorly, the fracture should be thought of as being open. High-energy injuries often are from motorcar accidents and occur in the young patient. These patients usually have associated accidents such as a hip fracture or dislocation or vascular or nerve damage. These high-energy injuries usually lead to comminuted fractures, principally of the metaphyseal area. Dedicated knee movies should at all times be obtained in the evaluation of distal femur fractures. In circumstances of extreme comminution, radiographs of the contralateral knee can aid in preoperative planning as properly. Patient with a distal femur fracture with intercondylar extension displaying the delicate rotational deformities of the individual condyles. The muscle forces are proven on the distal femur, as is the femoral artery and vein getting into the canal of Hunter (arrow). The adductor magnus inserts on the adductor tubercle, leading to a varus deformity of the distal section. A lateral picture of the same patient with the popliteal artery and tibial nerve drawn in to present the relative proximity to the fracture ends. Patient with a spiral distalthird femur fracture that appears to be extra-articular. Patient with a closed femur fracture that was initially thought to be extra-articular. Spinal twine injury (paraplegia or quadriplegia) Some particular conditions could warrant nonoperative care on case-by-case foundation. Nondisplaced or minimally displaced fracture Select gunshot wounds with incomplete fractures Extra-articular and steady Unreconstructable Lack of expertise by the obtainable surgeon or lack of kit or applicable facility to adequately deal with the harm. Transfer is indicated in these situations; otherwise, nonoperative treatment will be the only possibility. Skeletal traction Cast bracing Knee immobilizer Long-leg cast There are acceptable limits for nonoperative management: 7 levels of varus or valgus 10 degrees of anterior or posterior angulation. Once surgery is deemed acceptable for the patient and the particular injury, the surgical approach choices out there are determined by the particular fracture pattern. Treatment additionally must be determined based on components other than the classification alone. Simple intra-articular splits could also be treated with closed reduction and percutaneous fixation. The extra-articular damage ought to be handled using oblique discount strategies as a lot as possible to keep a biologic delicate tissue envelope. The surgeon should re-establish the length, rotation, and alignment of the femur and the limb. Fixation Choices External fixation A momentary bridging external fixator throughout the knee joint can be utilized if momentary stabilization is required before definitive fixation. This is normally the case where definitive open discount and inside fixation is deliberate.
3 pc vpxl
The obturator oblique view could be obtained by rotating the C-arm forty five levels toward a lateral view. Approach the posterior wall of the acetabulum is accessed via the Kocher-Langenbeck method. One begins on the posterior tip of the higher trochanter and extends distally alongside the posterior aspect of the femoral shaft, distal to the trochanter and the gluteal crease, which serves as an external landmark for the gluteus maximus tendon. The proximal limb extends about forty five levels towards a spot 1 cm cephalad to the posterior superior iliac spine. The size of this limb is dependent upon the amount of posterior column that must be accessed. The skin and subcutaneous tissue are divided all the way down to the fascia lata and the gluteal aponeurotic fascia. To open the proximal limb, the surgeon sharply divides the gluteal aponeurosis and then gently splits the gluteus maximus muscle through finger dissection. With the Charnley retractor in place, the surgeon excises the bursa if it obstructs visualization. The nerves that innervate the proximal third of the gluteus maximus will cross on this space, about halfway between the larger trochanter and the posterior superior iliac spine. The surgeon ought to stop splitting at the first nerve trunk to stop postoperative palsy. The Charnley retractor is helpful for holding the fascia away from the operative subject. The surgeon should take care not to insert too deeply to forestall iatrogenic harm to the sciatic nerve. This could be difficult owing to the situations of the traumatized tissues; typically will in all probability be best to determine the nerve in an space of healthy tissue, similar to at the degree of the quadratus femoris. If general visualization is insufficient at this point, the gluteus maximus tendon could be divided at its insertion on the femur. A cuff of tissue is left on the femur so an enough repair can later be performed. It could be useful to internally rotate the leg to put the short exterior rotators and the piriformis on stretch to help with identification. It is easier to palpate the edges of the piriformis tendon with a finger after which move a finger behind the tendon to better isolate it. The surgeon confirms that the proper muscle has been recognized by following its path backward and towards the larger sciatic notch. With the piriformis retracted, the sciatic nerve ought to now be easily visible, mendacity over the quick exterior rotators. Next, the surgeon identifies the tendon composed of the superior and inferior gemelli and the obturator internus. By pulling upward on this tag stitch�tendon, the surgeon can move a finger into each the greater and lesser sciatic notches, beneath the muscle, and due to this fact the nerve, making a path. In addition to defending the nerve, this helps to retract the soft tissues and provides glorious visualization of the retroacetabular surface. By retracting the gluteus medius anteriorly, the piriformis and obturator internus tendons are revealed. Piriformis and obturator internus tendons are tagged and launched from their insertion on the proximal femur. Retracting the piriformis allows identification of the sciatic nerve resting on the short exterior rotators. By utilizing the tag suture on the obturator internus tendon to retract it posteriorly, the sciatic nerve might be protected and safely retracted out of the operative area. By removing any residual hematoma from the field, the posterior wall fragment and the posterior column will become easily seen. The posterior column is inspected carefully for any nondisplaced transverse fracture line. The surgeon "books open" the fracture website by flipping the wall piece out into the wound.
6 pc vpxl cheap overnight delivery
The following clues may be necessary within the differential analysis: Sensation of giving means Effusion Atrophy of the quadriceps Tenderness over the joint line (or the meniscus) Reproduction of a click on by manipulative maneuvers in the course of the physical examination Probably an important physical finding is localized tenderness alongside the posteromedial or posterolateral joint line, which is most commonly brought on by reactive synovitis. A history of specific injury is in all probability not obtained, especially when tears of abnormal or degenerative menisci have occurred. A patient without locking sometimes offers a history of several episodes of hassle referable to the knee, often resulting in effusion and a short interval of incapacity however no definite locking. A sensation of giving method or snaps, clicks, catches, or jerks within the knee may be described, or the history may be much more indefinite, with recurrent episodes of ache and mild effusion within the knee and tenderness within the anterior joint space after extreme activity. The injured knee should be compared with the opposite knee, which may exhibit 5 to 10 levels of physiologic recurvatum. In this case, the injured knee could be locked and still lengthen to impartial place. False locking occurs most frequently quickly after an injury in which hemorrhage concerning the posterior a part of the capsule or a collateral ligament with associated hamstring spasm prevents complete extension of the knee. Effusion signifies that one thing is irritating the synovium; due to this fact, it has restricted specific diagnostic worth. The sudden onset of effusion after an harm often denotes a hemarthrosis, and it could occur when the vascularized periphery of a meniscus is torn. Tears occurring throughout the body of a meniscus or in degenerative areas might not produce a hemarthrosis. Repeated displacement of a pedunculated or torn portion of a meniscus can produce adequate synovial irritation to produce a chronic synovitis with an effusion of a nonbloody nature. Clicks, snaps, or catches, either audible or detected by palpation during flexion, extension, and rotary motions of the joint, may be priceless diagnostically, and efforts must be made to reproduce and accurately locate them. Numerous manipulative tests have been described, however the McMurray test is mostly used. For the McMurray check, with the knee completely flexed, the examiner palpates the joint line with one hand and uses the other hand to rotate the foot internally whereas extending the knee. If a meniscal tear is present, a click could additionally be heard or felt within the joint line of the affected facet during this maneuver. The grinding take a look at, as described by Apley, is another take a look at for isolating meniscal pathology. With the affected person susceptible, the knee is flexed to ninety levels and the anterior thigh is mounted in opposition to the analyzing desk. Next, with the knee in the same place, the foot and leg are pressed downward and rotated because the joint is slowly flexed and prolonged. Another useful test, the squat test, consists of several repetitions of a full squat with the toes and legs alternately fully internally and externally rotated because the squat is performed. Reproduction of ache on the medial or lateral aspect of the knee is suggestive though not diagnostic of meniscal tear. The analysis of inner derangement of the knee brought on by a meniscal tear may be tough to make even for an experienced orthopedic surgeon, but a cautious historical past and physical examination mixed with acceptable imaging research assist to limit errors in analysis and unnecessary arthroscopy. For simplicity, tears of the menisci are mentioned right here as if they had been isolated accidents, but evidence of different injuries all the time should be sought. Some have advocated total excision of torn menisci, whereas others have proposed subtotal excision. Justification for total excision often was based on shortterm, functional restoration standards; however, longer followup showed associated degenerative changes. Removal of even one third of the meniscus has been proven to increase joint contact forces by up to 350%. The quantity of degenerative change within the articular cartilage appears to be immediately proportional to the amount of meniscus eliminated. If meniscal pathology produces virtually daily symptoms, frequent locking, or repeated or continual effusions, the pathologic portion of the meniscus must be eliminated as a result of the problems brought on by the present incapacity far outweigh the chance or significance of future degenerative arthritis. Partial meniscectomy by arthroscopic technique has enough support and medical results to point out its routine use. Total meniscectomy is no longer thought of the remedy of choice in young athletes or different people whose daily actions require vigorous use of the knee. Small steady peripheral tears have been observed to heal after 6 to 8 weeks of safety. Stable vertical longitudinal tears, which are probably to occur within the peripheral vascular portions of the menisci, have been reported to heal with nonoperative therapy.
Diseases
- Pyknoachondrogenesis
- 3-methyl glutaconic aciduria
- BANF acoustic neurinoma
- Intrauterine growth retardation mandibular malar hypoplasia
- Immotile cilia syndrome, due to excessively long cilia
- Ohdo Madokoro Sonoda syndrome
- Palmer Pagon syndrome
- Spondylarthropathy
- Koone Rizzo Elias syndrome
Vpxl 12 pc effective
After drain placement, the wound is pulse lavaged and the rectus fascia is closed with operating heavy absorbable sutures. Care should be taken to not embody too many muscle fibers to avoid muscle necrosis. Interrupted sutures are used on the distal finish to present a side-to-side closure of the avulsed side. Reduction is confirmed under direct imaginative and prescient as well as on inlet and outlet views of the pelvis. For occasion, in tilt fractures a ball-spike can be used to push in opposition to the intact rami while pulling up the pubic body on the fractured side. Again, the C-clamp or an external fixator may be positioned to help approximate the pubic bodies to facilitate reduction with a Weber clamp. If fixation is tenuous or if the affected person turns into too sick to proceed with plating, an exterior fixator can always be added. Chemical modalities consist of unfractionated heparin, lowmolecular-weight heparin, vitamin K antagonists, and issue Xa indirect inhibitors. If patients have a contraindication for chemical prophylaxis secondary to another harm similar to a head bleed, an inferior vena cava filter ought to be considered. Our protocol consists of serial compression devices and subcutaneous heparin three times a day preoperatively. Once stable fixation is in place, patients must be off the bed to a chair within 24 hours of surgery if their overall situation allows. In general, practical outcomes correlate with the initial displacement of the damage. Patients with associated urologic accidents are at risk for urethral strictures, urinary tract infections, and even late infections. If it happens earlier and a lack of reduction happens, then revision osteosynthesis should be thought-about. Although no data exist, the quality of the initial discount seems to be the most effective predictor. Urologic complications embody late urethral strictures, incontinence, and erectile dysfunction. Early restore of bladder or urethral injuries on the identical time of fixation avoids more complex reconstructions, however the price of late urologic complications is still comparatively excessive. Separation of the symphysis pubis in affiliation with childbearing: a case report. Internal fixation in pelvic fractures and primary repairs of related genitourinary disruptions: a team approach. Kellam1 defined an enough reduction of anterior symphyseal widening as lower than 2 cm and reported that when this was obtained in rotationally unstable fractures, one hundred pc of sufferers returned to regular perform. Patients with posterior pathology had poor outcomes, with only 31% reporting normal operate. Pohlemann et al7 reported no residual posterior displacement in ninety five sufferers with type B fractures handled with anterior plating. This was related to an 11% incidence of late ache that occurred after exercise. Pohlemann et al7 additionally demonstrated type C accidents radiographically had more residual posterior displacement than sort B injuries. Only 33% of these type C patients have been painfree after combined anterior and posterior fixation. Intraoperative use of the pelvic C-clamp as an help in discount for posterior sacroiliac fixation. Innominosacral dissociation: mechanism of injury as a predictor of resuscitation necessities, morbidity, and mortality. Fractures and dislocations of the pelvis contain, in broad phrases, accidents to the anterior and posterior structures of the pelvic ring. Injuries to the anterior pelvic ring embrace symphyseal disruption and pubic body or rami fractures. The implications and treatment of injury to these constructions vary widely with the broad spectrum of injury patterns, combos of accidents, and degree of displacement. The two innominate bones are joined anteriorly on the pubic symphysis, a symphyseal joint.
1 pc vpxl buy free shipping
Drilling the assembled "Adapteur Drill Guide C-Ring with the Coracoid Drill Stop and Graduated Guide Pin Sleeve" (Arthrex, Inc. With the drill stop positioned on the base of the coracoid (as close to the scapula as possible), the corresponding space is marked on the superior facet of the clavicle for the information pin sleeve. Using the Adapteur Drill Guide C-Ring with the Coracoid Drill Stop beneath direct visualization, a guide pin is positioned by way of the clavicle and coracoid, engaging the drill stop. The pin should be centered on the clavicle and the coracoid and should exit the coracoid base as near the scapula as attainable. The surgeon should take care to cease at the drill stop and not advance previous the coracoid base. The power drill is indifferent and the cannulated drill is used as a portal to pass an 18-inch Nitinol suture passing wire. The limb of the Nitinol passing wire is brought out of the anteroinferior portal, leaving the loop superior to the clavicle. The Nitinol suture passing wire is used to deliver the white traction sutures through the clavicle and coracoid and out of the anteroinferior portal. While holding the blue TightRope suture tails, pulling on one of the white suture tails flips the oblong button to a vertical position, permitting passage of the TightRope by way of the clavicle and coracoid. Once past, independent pulling on the white sutures flips the rectangular button again to a horizontal position, anchoring it underneath the coracoid. Suture Passage and Tying the power drill is indifferent, leaving the cannulated drill in place. After discount of the clavicle, sequential pulling on the blue TightRope suture tails delivers the spherical button all the method down to the superior clavicle, holding the discount firmly. The blue TightRope suture tails of the spherical button are held firmly with one hand. Clavicle Reduction the surgeon pulls on the blue suture tails to advance the spherical button right down to the clavicle. An different is to displace the clavicle anteriorly with a towel clip to allow entry for conoid tunnel drilling. Graft administration Semitendinosus ends are bulleted to permit for straightforward graft passage. Sutures are passed under the coracoid either from medial to lateral or lateral to medial. If passing lateral to medial, the surgeon ought to make sure that the medial coracoid base is uncovered and will insert a Darrach retractor on the medial base to "catch" the passing system. When the ability driver is disconnected, the surgeon should pull the reamer out manually to make sure that the tunnel is a perfect circle and never widened by uneven reaming. The tenodesis screw is inserted anterior to the graft to equally recreate posterior coracoclavicular ligaments. These braces are really helpful to counter the pull on the shoulder complex by gravity. For the primary 6 to eight weeks, the brace could additionally be removed for grooming and supine mild passive vary of motion solely. Active and passive range-of-motion workouts are began at eight weeks after surgical procedure. If painless range of movement is obtained, power coaching is started at 12 weeks. Postoperative radiographs show that the mean difference within the coracoclavicular distance is 2. Weaver-Dunn Outcomes are difficult to evaluate due to the variations within the Weaver-Dunn method used and the make-up of the kind of patients and severity of damage within research teams. Arthroscopic reconstruction with the TightRope System: preliminary outcomes of an ongoing research: 29 sufferers with a mean age of 31 years and 6-month follow-up Mean Constant rating ninety one. Decision making: operative versus nonoperative remedy of acromioclavicular joint injuries.
12 pc vpxl buy with visa
Their symptoms are typically as a end result of distal embolization, acute thrombosis or compression of adjacent vein. The signs of acute limb ischaemia include pain, pallor, pulselessness, poikilothermia, paraesthesia and paralysis. A 55-year-old man presents with ache in his right calf muscular tissues when he walks one hundred m. On physical examination, he has palpable femoral pulses bilaterally however no palpable pedal pulses. The ulcer began after by chance injuring the skin around the nail mattress while she was clipping her toenails. On physical examination, the ulcer is three mm � 2 mm with a necrotic base and surrounding erythema. There are strong palpable femoral and popliteal pulses but no palpable pedal pulses. This normally happens with chronic arterial occlusive disease affecting the superficial femoral artery and/or popliteal artery. This often happens with tibial disease and is further confirmed by the presence of femoral and popliteal pulses and monophasic pedal indicators. A 51-year-old diabetic man presents with a 1 cm � 1 cm ulcer over the plantar facet of his proper great toe. The ulcer began as a blister after a chronic stroll carrying a new pair of footwear. Diabetic foot ulcers occur as results of steady stress at one spot within the setting of diabetic neuropathy. On bodily examination, he has a palpable pulsatile belly mass at the level of the umbilicus. He stopped smoking 1 year ago, has well-controlled hypertension and is in any other case in good health. A 59-year-old man presents with a historical past of a sudden onset of slurred speech associated with weak point in his proper upper extremity 2 hours previously. He is a chronic smoker and is understood to have stable coronary artery disease for which he receives medical therapy. The perfect initial imaging modality for diagnosing asymptomatic abdominal aortic and popliteal aneurysms is duplex ultrasonography, as a end result of its widespread availability, lack of radiation, low cost and reproducible results. This makes an ulcerated carotid plaque excessive on the list of differential diagnoses. It refers to morphological and useful venous disorders with scientific manifestations various from easy superficial venous dilation to venous hypertension with chronic pores and skin changes and ulceration. Chronic venous disease often begins as a outcome of venous valve dysfunction, venous pump failure or venous obstruction. Over time, a build-up of pressure inside the venous system directs the blood move abnormally from the deep to the superficial venous system, which in turn could lead to skin fibrosis, native inflammation and ulceration. There are many threat elements for the event of venous disease, together with advancing age, a family historical past of venous pathology, an elevated physique mass index, prolonged standing, smoking, prior venous thrombosis and being pregnant. Competent valves forestall retrograde circulate into the superficial venous circulation, and the venous strain of the superficial circulation is maintained at between 20 and 30 mmHg during ambulation. Presentation Chronic venous illness encompasses a large spectrum of useful and morphological venous problems, and as such its clinical manifestations vary significantly. Pain and oedema are sometimes worse when the affected person is standing or when the ft are in a dependent place for prolonged intervals of time; this usually improves with limb elevation. Nevertheless, the signs are often extra prominent at night when the affected person goes to bed. Numbness and tingling may also be current however are tough to differentiate from other causes of peripheral neuropathy in the leg. Some patients complain of cramping, itching and swelling, and this is usually related to persistent skin modifications. Skin ulceration and bleeding of varicose veins are often late manifestations of severe venous reflux illness. The physical findings are also variable and normally correlate with the severity of the symptoms. Telangiectasias, that are small dilated intradermal veins, are often early manifestations of venous illness.
Cheap 1 pc vpxl otc
The release is continued medial alongside the posterolateral coracoid till the subscapularis muscle belly is seen beneath the arch of the coracoid neck and base. A 30-degree arthroscopic elevator, launched via an anterosuperolateral portal, is used to perform the superior launch, lysing adhesions between the subscapularis and the coracoid neck and base. The release is finished solely to the midpoint of the undersurface of the coracoid neck (to prevent harm to the neurovascular buildings medial to the coracoid neck). The inferior launch is probably the most dangerous and has not been necessary in our expertise. A ring curette may be used to exactly take away the delicate tissues as much as the articular margin. An electrocautery probe is used to delineate a medialized footprint on the lesser tuberosity (A), and a power burr burrs off the "charcoal" down to bleeding bone (B). This skeleton exhibits how the arm is held in 20 to 30 degrees of abduction and 20 degrees of forward flexion during shoulder arthroscopy in the lateral decubitus position. Photograph from the head wanting downward reveals how the mixture of abduction, forward flexion, and regular humeral retroversion necessitates a "hand on face" place throughout anchor insertion into the lesser tuberosity. This "hand on face" place allows the surgeon to obtain an acceptable "deadman" angle to insert suture anchors into the lesser tuberosity. The anchors should be placed so as from inferior (caudal) to superior (cephalad). One strand of suture is retrieved from the anchor, pulled out the anterosuperolateral cannula, and loaded within the suture passer. For the superior anchor, the sutures must be passed over the top of the superolateral border of the subscapularis, simply medial to the "comma tissue. The double-diameter knot pusher permits the subscapularis tendon to be manipulated and held in the appropriate position whereas each halfhitch of the knot is tied. Sutures from the upper anchor have been positioned at the junction of the vertically oriented comma tissue and the upper border of subscapularis tendon. Proper portal placement is imperative to achieve the proper angle of method to work within the subcoracoid area. The key rules embody minimizing pressure differentials (hypotensive anesthesia with adequate arthroscopic pump pressure), avoiding turbulence, utilizing the posterior lever push, and using both the 30- and 70-degree arthroscopes freely. The subscapularis tendon should be securely apposed to the bone to optimize therapeutic. Important biomechanical rules embody the correct angle of insertion of the suture anchors; use of double-loaded anchors to scale back the load on every suture; use of strong sutures; correct suture placement within the tendon; and optimized loop and knot safety. The patient should clearly understand what he or she can do to defend and optimize healing of the subscapularis tendon restore. After the arthroscopic portals are closed, a sterile dressing is utilized over the shoulder. During the primary 6 weeks the affected person ought to perform daily lively wrist and elbow motion. The patient must not externally rotate past neutral (straight-ahead position) for six weeks. The patient is started on a passive stretching program that includes passive exterior rotation with a cane up to 45 degrees and overhead stretches with a rope and pulley. At 12 weeks from the operation the affected person is started on a strengthening program with elastic bands. If the subscapularis tear is part of a large anterosuperior rotator cuff tear, then strengthening is delayed until sixteen weeks postoperatively. Rehabilitation focuses on strengthening the scapular stabilizers and deltoid and rotator cuff muscles. Eight of ten sufferers who had proximal humeral migration preoperatively had reversal of the migration and useful overhead use of their arm. Bennett2 additionally found encouraging leads to his potential cohort with 2- to 4-year follow-up.
Curtis, 37 years: Restoration of regular muscular perform through using low-impact exercices is emphasised during weeks 9 by way of 16. Patients should have no much less than three units of typed and cross-matched blood on maintain. An inferior-to-superior course is used for this maneuver to achieve a small capsular plication.
Kliff, 26 years: Metal fixation options embody lag screws, variable pitch fully threaded screws, or Kirschner wires (less compression). Stability of posterior fracture-dislocations of the hip: quantitative evaluation using computed tomography. The doctor ought to identify open fractures and establish the "persona" of the injury.
Pranck, 63 years: They could be introduced via the fracture website into the proximal fragment in a retrograde trend or into the distal fragment in an antegrade style. It is the remnant of the medial sling of the biceps after it pulls loose from its footprint on the lesser tuberosity instantly adjoining to the footprint of the higher subscapularis. Definitive administration with bridging or nonbridging external fixation can be used for unreconstructable joints, very severe gentle tissue accidents, or extreme osteopenia.
Cobryn, 56 years: Vascular malformations can have an effect on the capillaries, venous system or lymphatic system. In the initial phase, emphasis is placed on regaining full motion, controlling effusion, and sustaining quadriceps tone. Surgical violation of the iliopsoas tendon carries the danger of heterotopic ossification, in either an open or arthroscopic procedure.
Akrabor, 57 years: Intestinal peristalsis pushes the internal loop additional and further down, leading to the intestinal obstruction. The arthroscope is placed into the suprapatellar pouch with the knee in extension. Areas of swelling or ecchymosis, breaks in the integument, and the presence or absence of fracture blisters must be identified and documented preoperatively.
Esiel, 23 years: Intra-abdominal Abscess Intra-abdominal abscesses could develop as the end result of an infectious process. Lateral-row suture anchor placed at the lateral facet of the larger tuberosity between the 2 medial-row anchors. Medial meniscus the medial meniscus covers a smaller proportion of medial compartment surface than the lateral meniscus.
Dan, 49 years: Increased fatty infiltration of the rotator cuff muscular tissues has been correlated with poorer tendon healing and worse last postoperative outcomes after repair. This will guarantee a watertight seal for the implanted chondrocytes beneath the periosteum graft. Subtrochanteric femoral shaft fractures Percutaneous remedy compared to plating methods.
Diego, 21 years: The restoration of the mechanical axis may be checked intraoperatively after temporary stabilization (preferred) or definitive stabilization using the Bovie wire. Medial deviation of the guidewire will lead to abutment towards the steep medial cortex and result in valgus angulation at the fracture site with nail insertion. Damage to the nerves, muscle and connective tissues of the pelvic floor throughout childbirth might be the most typical reason for stress incontinence.
Killian, 38 years: The two mostly used techniques are the Whiteside aspect port needle and the slit catheter device. Their work documented that the radial nerve averaged 7 mm from the arthroscope sheath when the elbow was flexed ninety levels. The impact of manipulation beneath general anesthesia: structure and glycosaminoglycan content material of the joint capsule.
Shawn, 52 years: The peroneal department is tested with ankle and toe dorsiflexion and sensation on the highest of the foot. The stability of the lesion and the intergrity of the overlying cartilage can be assessed immediately. Chapter 13 Arthroscopic Acromioclavicular Joint Reduction and Coracoclavicular Stabilization: TightRope Fixation Michael S.
Redge, 29 years: Patients with perianal warts normally complain of itching, bleeding and perianal lumps; there can also be signs from warts elsewhere on the genitalia. The perineal post is pictured right here within the perineum, which is best for proximal fractures. Iliotibial band the varied open approaches use a typical, lateral, longitudinal incision over the larger trochanter.
Brant, 44 years: Alternatively, autogenous semitendinosus and gracilus grafts could be harvested (see Chap. Other causes embrace urethral harm associated with penile fracture, and iatrogenic injury during instrumentation and catheterization. Aglietti et al12 famous radiographic therapeutic in 16 knees, and all patients had been asymptomatic at follow-up of four years.
Aidan, 27 years: The tenodesis driver is superior to touch the tendon graft, and the entire tendon, driver, and screw advanced is positioned into the coracoid bone tunnel until 15 mm of the Krakow suture disappears. However, some patients develop severe signs requiring hospitalization and intravenous therapy. These include: � � � � � nerve root lesions similar to pre-eruption herpes zoster; diabetes; hyperparathyroidism; porphyria; tabes dorsalis, which is a form of syphilis.
Porgan, 25 years: Such sufferers persistently submit themselves to surgical procedure and invasive procedures for the situation they simulate. Perform an arthroscopic d�bridement and excoriation to the far peripheral meniscal rim or joint capsule with a shaver or meniscal rasp. Abdominal distension could develop due to ileus, leading to hyperresonance, and later be augmented by ascites, resulting in dullness on percussion.
Garik, 39 years: The most common causes of large bowel obstruction are colon most cancers, incarcerated hernia, sigmoid or caecal volvulus, faecal impaction and diverticular strictures. The graft is positioned so that the graft tail representing the conoid ligament is left 2 cm proud from the superior margin of the clavicle. An various is to displace the clavicle anteriorly with a towel clip to allow access for conoid tunnel drilling.
Arokkh, 61 years: Strengthening and gait coaching will start at this time, with special focus on the hip abductors. The rigid reamer want only open the highest of the bone for entry to medullary canal. Careful inspection could reveal atrophy in the supraspinatus and infraspinatus fossa in comparison with the opposite side.
Wilson, 47 years: With proper diagnosis, the surgical results for snapping of the iliopsoas tendon and the iliotibial band are highly predictable and finite when it comes to decision of the snapping. However, return of ache and failure are related to osteochondral lesions larger than 2 cm in diameter. Full assessment of the lesion was not accomplished till the defect was d�brided to secure rim.
Elber, 46 years: The anterior capsule is taut in extension and lax in flexion, with the strength of the capsule supplied from the cruciate orientation of the fibers of the anterior capsule. Embryologically, the omphalomesenteric duct, linked to the midgut, and the urachus, linked to the bladder, are the weather of the umbilical cord. The function of the posterior cruciate is to resist posterior tibial translation of the tibia relative to the femur.
Yasmin, 65 years: Clostridial and different anaerobic organisms (gas gangrene) could have an effect on the superficial and deep fascia and the muscle layers, or the complete wall. Effect of impression on chondrocyte viability during insertion of human osteochondral grafts. A lack of passive inner rotation suggests contracture of the posterior capsule.
Chenor, 48 years: Sacral foraminal and central spinal canal involve- ment is confirmed, as is integrity of the posterior pressure band. Screw size measurement could be confirmed with a frogleg lateral or a real lateral view with flexing of the hip to clear the contralateral leg. Steatorrhoea, weight loss and new-onset diabetes occur with pancreatic endocrine and exocrine insufficiency.
VPXL
10 of 10 - Review by G. Will
Votes: 261 votes
Total customer reviews: 261
10 of 10 - Review by G. Will
Votes: 261 votes
Total customer reviews: 261
References
- Kim YT, Kwon DD, Kim J, et al: Gabapentin for overactive bladder and nocturia after anticholinergic failure, Int Braz J Urol 30(4):275, 2004.
- Amparo EG, Hoddick WK, Hricak H, et al: Comparison of magnetic resonance imaging and ultrasonography in the evaluation of abdominal aortic aneurysms, Radiology 154:451-456, 1985.
- Smith CL, Gemar SK, Lewis MJ: Pseudoephedrine urolithiasis associated with acute renal failure, Nephrol Dial Transplant 19(1):263n264, 2004.
- Douglas J:ADescription of the Peritoneum, and of that Part of the Membrana Cellularis Which Lies on Its Outside.With an Account of the True Situation of All the Abdominal Viscera, in Respect of These Two Membranes. J Roberts, London, 1730.
- Bagley, D.H., Rittenburg, M.H. Intrarenal dimensions. Guidelines for flexible ureteropyeloscopes. Surg Endosc 1987;1:119-121.
- Kanatous SB, Garry DJ. Gene deletional strategies reveal novel physiological roles for myoglobin in striated muscle. Respir Physiol Neurobiol. 2006;151(2-3):151-158.
- Ellis SG, et al: Facilitated PCI in patients with ST-elevation myocardial infarction. N Engl J Med 2008;358:2205-2217.
